
HGE
. For patients with diagnosis as dyspepsia, they may have many symptoms. Which of the following symptoms is the most likely encountered?
A. Upper abdominal fullness
B. Diarrhea
C. Dysphagia
D. Hematemesis
E. Constipation
. For the patient you consult for dyspepsia, you have to do anamnesis and clinical examination to find the causes. Which of the following etiology that is the most likely play a role?
A. Insomnia
B. Alcohol
C. Helicobacter pylori Infection
D. Intestinal parasite
E. Smoking
Some drugs can cause dyspepsia. So during your anamnesis for patient with dyspepsia, you have to think of some drug name. What medication is the most likely responsible?
A. Aspirin, NSAIDs
B. Amitriptyline
C. Paracetamole
D. Steroid
E. Metronidazole
. Rome III diagnostic criteria are used to diagnose functional dyspepsia. Which one of the following propositions is based for Rome criteria?
A. Clinical criteria
B. Severity of symptom
C. Early response to treatment
D. Blood test
E. Abdominal ultrasound
Q5. In case of dyspepsia, we have to find some alarm features (“Red flags"), which is suggestive of gastric malignancy. Which one among the following propositions is the most appropriate?
A. Age > 50 years with new-onset dyspepsia
B. Symptom not response to treatment
C. Sleep disturbance
D. Severity of pain
E. Long history of pain
Q6. A patient of 55 years old comes to see you for symptoms of dyspepsia. Anamnesis and clinical examination revealed that he lost 5 kg for the past 2 months and his father died of gastric cancer so you have to diagnose whether the patient was infected by H. Pylori. Which of the following tests would you think is the most appropriate?
A. Gastroscopy + histology
B. Gastroscopy + rapid urease breath test
C. H. Pylori stool test
D. H. Pylori serology
E. H. Pylori in saliva
Q7. The co-factors of irritable bowel syndrome can be related to many factors. Which one of the following factor is the most likely play a role?
A. H. Pylori infection
B. Colitis
C. Peptic ulcer
D. Dietary factors
E. Serious infection
Q8. In patients with irritable bowel syndrome, symptom for which we have to look for in the alarm features were below. Which of the following propositions is the most likely?
A. Age > 50 years with long onset of symptoms
B. Unremitting or Nocturnal symptoms
C. Past history of parasitic infection
D. Intentional weight loss
E. Severity of symptom
Q9. In people who meet the IBS diagnostic criteria, the following investigations are recommended. Which of the following para-clinic exams is the most likely requested as minima?
A. Colonoscopy
B. Abdominal scanner
C. Abdominal ultrasound
D. Full blood count (FBC or CBC)
E. Lipasemia
Q10. A patient of 45 years old comes to see you for symptom of irritable bowel syndrome about 2 months. He has rectal bleeding one to two times weekly. Which investigation is the most likely diagnostic?
A. Anuscopy
B. Colonoscopy
C. Gastroscopy
D. Abdominal scanner
E. Abdominal ultrasound
Monsieur X., âgé de 58 ans, est hospitalisé au service urgence pour une hématémèse. A l’examen clinique: la tension artérielle est de 100/60mmHg avec la fréquence cardiaque à 110/min, les téguments et muqueuses sont pâles. Il présente un ictère, des angiomes stellaires sur le tronc et des circulations veineuses collatérales. L’abdomen est distendu avec la matité déclive avec splénomégalie. TR : méléna. Quel diagnostic étiologique le plus probable évoquez-vous?
Oesophagite ulcéré complique
Syndrome de Mallory-Weiss
Rupture des Varice œsophagienne
Ulcère gastroduodénal complique
Saignement par d’Angiodyspalsie
Un patient âgé de 66 ans est hospitalisé pour une hématémèse. A l'interrogatoire, vous notez qu'il a de l'hématémèse 3fois. Comme l'antécédent: l'infarctus du myocarde il y a 3mois. A l'examen clinique: TA: 98/72mmHg, FC: 100/mn, absence de marbrure. Quel critère de gravité de ce patient que vous inquiétez le plus?
Age du patient
Co-morbidité du patient
Nombre de l'hématémèse
Etat hémodynamique
Cause de l'hémorragie
Mme Y. âgée de 40ans est hospitalisée pour une hémorragie digestive haute. Elle a la notion de la prise de l'ANIS depuis 5jours. Elle a bénéficié d'une endoscopie haute qui a montré un ulcère gastrique Forrest IIb. Quelle hormone de la défense de muqueuse gastrique qui est perturbé lors de l'utilisation de l'AINS?
Gastrine
Prostaglandine
Histamine
Somatostatine
Sécrétine
Un homme de 60 ans ayant antécédent familial de cancer colorectal, est admis au service urgence porte pour une rectorragies massives. A l'examen clinique: TA: 90/60mHg, FC: 120/mn, le tégument et muqueuse sont pâle et le reste de l'examen est normal. Quel est le premier examen paraclinique à visée diagnostique et thérapeutique à faire?
Coloscopie
Gastroscopie
Angiographie
Echographie
Rectoscopie
Une femme de 40 ans est admise dans le servie de l’hépato-gastroentérologie pour une hématémèse. Elle a bénéficié d'une endoscopie oeso-gastroduodénale qui a montré un grand ulcère gastrique Forrest Ib. L'hémostase endoscopique a été réalisée. Quel est le traitement médical le plus approprie proposez-vous?
ESOMEPRAZOLE 50mg en bolus puis 40mg en intraveineuse une fois sur 24h
ESOMEPRAZOLE 40mg en bolus puis 40mg intraveineuse deux fois sur 24h
ESOMEPRAZOLE 80mg en bolus puis 8mg/h en intraveineuse sur 24h
ESOMEPRAZOLE 80mg en bolus puis 40mg en intraveineuse une fois sur 24h
ESOMEPRAZOLE 50mg en bolus puis 25mg/h en intraveineuse sur 24h
Le 16/11/2014, 20h40, Vous êtes interne au service urgence porte d’un hôpital à Phnom Penh. Monsieur C.V, âgé de 53 ans amené par son fils pour une émission de selle noirâtre une fois à 17 heures. Question 16 (QRU) 20h42, vous avez un doute sur ce méléna à l’interrogatoire. Quel est le geste le plus approprie que vous devez faire pour le confirmer ?
Endoscopie rectal
Toucher rectal
Coloscopie
Sonde rectale
Lavement rectal
Le 16/11/2014, 20h40, Vous êtes interne au service urgence porte d’un hôpital à Phnom Penh. Monsieur C.V, âgé de 53 ans amené par son fils pour une émission de selle noirâtre une fois à 17 heures. Question 17 (QRU) 20h45, l'hémorragie digestive est confirmée après votre examen. La tension artérielle est à 80/40mmHg, FC 110/mn, FR 22/mn, SpO2 96% en air ambiant, la température à 370C, Glasgow 15. Vous reprenez votre interrogatoire minutieux, vous avez noté que c’est le premier épisode de méléna. Il n’en a pas de l’antécédent médical, chirurgical ou familial connu. Il n'a jamais pris de médicament. Il n’a pas d’allergie connue. Il fume 1 paquet par jour et il boit du vin du riz 1 litre par jour depuis l’âge de 30 ans. A l'examen clinique, vous avez trouvé des angiomes stellaires, circulation veineuse collatérale avec ictère conjonctival. Quel type de médicament le plus utile prescrivez-vous pour ce patient?
Bêtabloquant
Vaso-actif
Hémostase systémique
Inhibiteur de la pompe à protons
Antifibrinolytique
Le 16/11/2014, 20h40, Vous êtes interne au service urgence porte d’un hôpital à Phnom Penh. Monsieur C.V, âgé de 53 ans amené par son fils pour une émission de selle noirâtre une fois à 17 heures. Question 18 (QRU) 21h00. Après votre prise en charge immédiate l'état hémodynamique du patient est stable. Le patient a bénéficié d'une endoscopie en urgence qui montre de trois cordons variqueuse oesophagienne de stade III avec des signes rouge. La ligature élastique a été réalisée. Votre sénior vous a demandé, pourquoi existe-il des varice oesophagiennes pour ce patient?
Insuffisance hépatocellulaire
Hypo albuminémie
Hypertension portale
Rétention hydro sodée D
Trouble de coagulation
Le 16/11/2014, 20h40, Vous êtes interne au service urgence porte d’un hôpital à Phnom Penh. Monsieur C.V, âgé de 53 ans amené par son fils pour une émission de selle noirâtre une fois à 17 heures. Question 19 (QRU) 21h30. La ligature des varices oesophagiennes a été réalisée avec succès. Quels types de traitement prescrivez-vous pour la prévention de l'encéphalopathie chez ce patient?
Lactulose
Antibiotique
Bêtabloquant
Diurétique D
Albumine
Le 16/11/2014, 20h40, Vous êtes interne au service urgence porte d’un hôpital à Phnom Penh. Monsieur C.V, âgé de 53 ans amené par son fils pour une émission de selle noirâtre une fois à 17 heures. Question 20 (QRU) Le lendemain, le patient allait mieux. Il n'existe pas de désorientation temporo-spatiale. A l'examen clinique vous trouvez de l'ictère, des angiomes stellaires, d'ascite de moyenne abondance avec des circulations veineuses collatérales. Le bilan biologique: Hb: 80g/L, VGM : 84,7 fl, GB : 8,39giga/l, Plaquettes : 85 giga/l. Transaminase: ASAT: 3 fois à la normal et ALAT: 2 fois à la normal. Urée et créatinine sanguine sont normales. L'échographie a confirmé la cirrhose du foie chez ce patient. Votre sénior vous demande de faire le bilan biologique pour calculer le score de Child-Pugh. Quel est la proposition la plus appropriée pour calculer ce score?
Alpha foeto-protéine, INR, Albumine
Taux de prothrombine, Bilirubine total, Albumine sérique
Alpha foeto-protéine, Taux de prothrombine, Bilirubine totale
INR, Bilirubine totale, Taux de prothrombine
Taux de prothrombine, Bilirubine total, Albumine de liquide d'ascite
Monsieur CX âgé de 30ans se présent au Service des urgences porte pour douleurs épigastriques intense transfixant intermittente calmée par la position antéflexion avec vomissements et l’ arrêt des matières. Dans son antécédent: plusieurs épisodes de ce type de douleur mais régressée spontanément. Une ASP a montré de quelques calcifications à la région épigastrique sans image hydro-aérique ni croissance gazeux. Quel est le diagnostic le plus probable de ce patient?
Tumeur du pancréas
Pancréatite chronique
Ulcère gastrique
Infarctus du myocarde
Colique néphrétique
Madame XG âgé de 44 ans divorcé 10ans, elle boit beaucoup de la bière depuis la séparation avec son marie. Le diagnostic de la pancréatite chronique est porté il y a 6mois. Récemment, elle a des vomissements post prandiaux avec sensation d’un gène épigastrique. L'échographie ne montre pas des anomalies particulières sous réserve de gaz abondance. Mais vous avez encore le doute sur le pseudo-kyste du pancréas. Vous êtres a l’hôpital Calmette, quel examen para-clinique le plus adapte demandez-vous dans ce cas?
Echo-endoscopie
Scanner abdominal
IRM pancréatique
CPRE
Gastroscopie
Vous faite la visite matinale avec votre senior, vous s'occuper d'une dame de 54ans ayant la pancréatite chronique. La patiente a des vomissements répètes, Ceux-ci sont dues aux complications de la pancréatite chronique. Quelle complication la plus probable est responsable de vomissements répétés chez cette patiente?
Carence de la vitamine
Destruction de la cellule bêta
Douleur pancréatique
Destruction de la cellule exocrine
Pseudo-kyste du pancréas
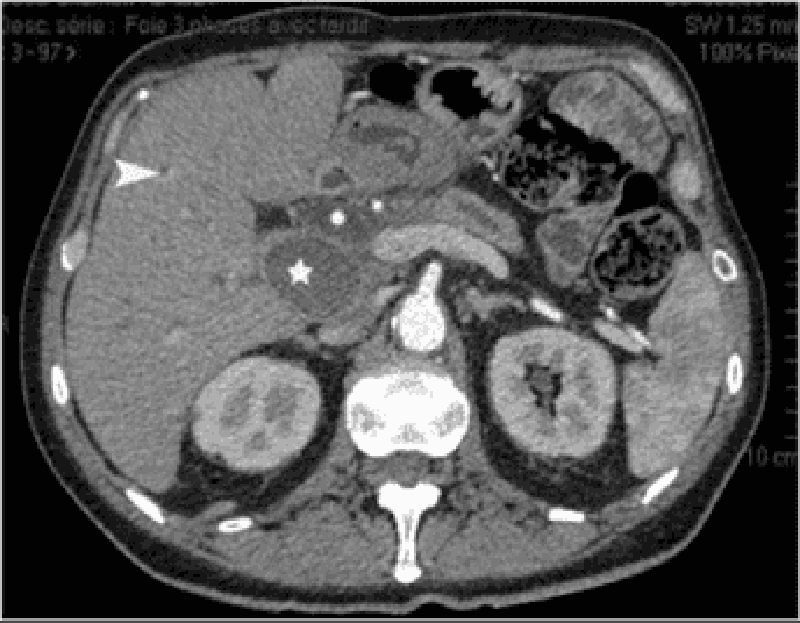
Lors d'un bilan scannographique du Monsieur TG âgé de 39ans pour l'ictère, on a découvert fortuitement d'un pseudo-kyste du pancréas de taille 30x40mm. Quelle est la cause possible de cet ictère?
Compression des voies biliaires intra-hépatiques
Compression du canal de Wirsung
Compression des canaux de Santorini
Compression de la voie biliaire principale
Compression du duodénum
Monsieur XK âgé de 56ans ayant la pancréatite chronique. Il a la douleur quant il mange n'import quoi. Il vient vous voir pour le régime. Quelle est la meilleure recommandation pour lui?
Régime pauvre en sucre et pas d'alcool
Régime hyposodé et pas de l'eau gazeux
Régime pauvre en graisse et pas d'alcool
Régime pauvre en protide et pas de l'eau gazeux.
Régime pauvre en sucre et pas de l'eau gazeux
Question 26 Vous avez vu en consultation Mme TX âgée de 56ans ayant un adénocarcinome du pancréas avec métastase hépatique. L'état général est bon sans syndrome de cholestase biologique. Quel traitement le plus approprie faite-vous pour cette dame?
Résection et radiothérapie
Chimiothérapie et radiothérapie
Résection et chimiothérapie
- Double dérivation et radiothérapie
Chimiothérapie et nutrition
Question 27 Monsieur JF âgé de 61ans ayant une altération de l'état général. Le bilan complet a montré une tumeur de tête du pancréas (30mm) de type adénocarcinome sans envahissement locorégional ni métastase à distance. Quel est le taux de survie à 5ans pour ce patient s'il est d'accord pour l'opération?
5 à 10 %
10 à 20 %
40 à 50%
30 à 40%
20 à 30%
Question 28 Monsieur CR âgé de 45ans est admis au service de Médicine A4 de l'hôpital Calmette pour un doute d'une tumeur du pancréas. Votre confrère vous a contacté et vous a posé la question: quel examen complémentaire le plus performance dans le carde de diagnostic d'un adénocarcinome du pancréas ?
Marqueuse tumorale Ca19.9
Scanner abdomino-pelvien
Echo-endoscopie pancréatique
Pet-scan au FDG
IRM abdomino-pelvien
Question 29 Madame TS âgée de 54ans avec notion familial de cancer du pancréas. Elle vous demande quels sont les symptômes faisant évoquer une tumeur du pancréas?
Amaigrissement et jaunice avec selles décolorées
Douleur de l'épigastre et diarrhée avec selles glaireuses
Amaigrissement et vomissement post prandial
Douleur de l'hypochondre droit et jaunice avec vomissement
Amaigrissement et selle glairo-sanglant
Question 30 Un patient âgé de 60ans ayant un adénocarcinome de la tête du pancréas est hospitalisé au service d'urgent pour l'état fébrile. Quelle est la cause qu'on doit rechercher en premier intention ?
Angiocholite
Occlusion intestinal
Diarrhée hydrique
Perforation intestinal
Pneumopathie infectieuse
QUESTION 31. The most frequent cause of UGI bleeding is:
. Esophageal varices
Peptic ulcer disease
Angiomata
Mallory Weiss tear
Gastritis
QUESTION 32. After initial stabilization and resuscitation of the patient, each of the following options should be considered in the management of UGI bleeding except:
Determine the source of bleeding
Stop acute bleeding
Treat the underlying abnormality
Prevent rebleeding
Emergency surgery
QUESTION 33. Endotracheal intubation for airway protection in the management of UGI bleeding should be considered:
In all cirrhotic patients
In all patients with UGI bleeding
In patients with altered mental status and ongoing hematemesis
In patients with stable COPD
Unless it delays urgent endoscopy
QUESTION 34. A 73 year old man presents with several episodes of hematemesis. Examination shows signs of orthostatic hypotension and melena. What is the first priority in caring for this patient?
Nasogastric tube placement and gastric lavage
Resuscitation with adequate IV access and appropriate fluid and blood product fusion
Intravenous infusion of H2-receptor antagonists to stop the bleeding.
Urgent upper panendoscopy
Urgent surgical consultation
QUESTION 35. An important risk factor for peptic ulcer hemorrhage includes:
Gastric acid hypersecretion
. Corticosteroid use
. Cigarette smoking
Non-sterioidal anti-inflammatory drug use
Ethanol consumption
QUESTION 36. For the patient who is now stable after a severe UGI bleed associated with NSAID ingestion, and who is found to be H.pylori positive, what is the most effective management strategy?
Stop NSAIDS, eradicate H.pylori, PPI therapy IV
Stop NSAIDs, full dose H2RA or daily PPI maintenance therapy
Stop NSAIDs
Eradicate H.pylori, full dose H2RA or daily PPI maintenance therapy
. Full dose H2-receptor antagonist or daily PPI maintenance therapy
QUESTION 37. For the patient with an UGI bleed and the endoscopic finding of a clean ulcer, the most appropriate management includes:
Endoscopic hemostasis with multipolar or heater probe or injection treatment
Endoscopic hemostasis with combination therapy
Emergent surgery
Medical therapy, early refeeding, same day discharge if stable(medically) and reliable
Medical therapy alone in a monitored setting for three days
QUESTION 37. A sixty-six-year old man presents to the emergency department with a history of one episode of melena. Past history includes coronary artery disease, hypertension . He is on one baby aspirin daily. An urgent upper endoscopy is negative. What is the most appropriate next step?
UGI series with small bowel follow-through
Colonoscopy
Angiography
. Red blood cell tagged technetium scan
Abdominal CT scan with contrast
QUESTION 38. A fifty-eight year old female patient presents to the emergency department with a 24-hour history of several hematemesis. She is found to be hypotensive and anemic. Resuscitative measures are instituted. What is the most appropriate next step?
Urgent gastroscopy
Anoscopic examination
Colonoscopic examination
Scintigraphy
Angiography
QUESTION 39. A fifty-eight year old female patient presents to the emergency department in Calmette hospital with a 24-hour history of several hematochesia. Physical examination show: hypotension, and anemia. Both the upper endoscopy and colonoscopy are not diagnostic. The patient continues to pass clots per rectum. Resuscitation has normalized her vital signs and maintained her Hct at 32%. What is the most effective management strategy?
Abdominal CT scan with contrast
Magnetic resonance imaging
Scintigraphy and angiography
Emergency surgery with intraoperative enteroscopy
Barium enema
QUESTION 40. A 65-year-old woman has a prior history of hospitalization for UGI bleeding from a duodenal ulcer. Which one of the following therapies is not useful for preventing recurrent ulcer hemorrhage?
Long-term maintenance therapy with full dose H2RA or daily PPI
H. Pylori eradication
Discontinuation of NSAID intake
Ulcer surgery
Bland diet
QUESTION 41. A 68-year-old healthy woman with a history of duodenal ulcer is placed on low-dose aspirin for coronary prophylaxis. Two weeks later she presents to the emergency room in Calmette hospital with one episode of melena . Physical examination showed : blood pressure and resting heart rate of 90 beats per minute without orthostatic changes. Melena is confirmed on rectal examination. Her admission hematocrit is 36%. She is placed on high dose proton pump inhibitor therapy (omeprazole 40 mg b.i.d.). Due to other complications, endoscopy is not performed until the tenth hospital day, and it shows a small (5 mm) duodenal ulcer with a clean base. Biopsy for CLO test is negative. Which one of the following should be performed now?
Treat with misoprostol for an NSAID-related ulcer
. Treat empirically with antibiotics for H. pylori
Obtain serum gastrin level to exclude Zollinger-Ellison syndrome
. Perform another test to exclude H. pylori
. Continue high-dose proton pump inhibitor therapy
QUESTION 42. A 32-year-old female presents with her third episode of symptomatic peptic ulcer. She has previously undergone multiple upper endoscopies, which have shown a non healing-benign-appearing antral ulcer. Multiple biopsies have always been negative for malignancy and gastritis. H. Pylori testing with both CLO tests and stool antigen are negative. Serum gastrin is normal. Which one of the following should be considered now?
Antrectomy
Serum salicylate level
High dose misoprostol therapy
High dose H2 receptor antagonist therapy
Sucralfate therapy
QUESTION 43. An 82-year-old debilitated woman with coronary artery disease and breast cancer presents with hematochezia requiring 4 units of blood. Following colonic preparation, colonoscopy demonstrates fresh blood in the left colon with marked diverticulosis. The right colon is normal and bilious material is seen in the cecal pole. Upon withdrawal of the colonoscope, there was active oozing of blood from the neck of a diverticulum in the distal sigmoid colon. The most appropriate management now is
Supportive care with transfusion requirements as necessary
Technetium RBC scan
Angiography
Endoscopic therapy of the bleeding diverticulum
Immediate surgical therapy
Question 44. A 65-year-old presents with iron-deficiency anemia, refractory to iron treatment. No history of overt gastrointestinal bleeding, but fecal occult blood tests were positive on 4 of 5 occasions. A previous EGD showed a large hiatal hernia. Two colonoscopies and a small bowel radiographic series were unremarkable. An endoscopic finding of a repeat EGD is shown ulcerative esophagitis. Which of the following is the most appropriate management of this condition?
Endoscopic ligation
Endoscopic sclerotherapy
. Laparoscopic Nissen fundoplication
Distal esophagectomy
Oral administration of a proton pump inhibitor twice daily and iron replacement therapy
Question 45. A 72-year-old woman with cryptogenic cirrhosis has developed progressive dyspnea for the past 3 months. Her laboratory investigations show hemoglobin of 8.4 g/dL with mean corpuscular volume of 62 μm3 and serum ferritin level of 10 ng/mL. Stool specimens are brown but positive for occult blood. Colonoscopy is normal. An endoscopic view of the gastric antrum is shown Angiodysplasia. Which of the following is the most appropriate next step in management of this condition?
Partial gastrectomy or antrectomy
Argon plasma coagulation
Transjugular intrahepatic portosystemic shunts (TIPS)
. Oral administration of proton pump inhibitors twice daily
Oral administration of non-selective beta-blockers
Question 46. A 62-year-old woman with a past medical history of chronic renal insufficiency presents with iron-deficiency anemia and intermittent melena for 2 months requiring multiple blood transfusions. She underwent multiple endoscopic investigations, including EGD, colonoscopy, CT scan of the abdomen and pelvis, and upper gastrointestinal series. No bleeding source was identified. Wireless capsule endoscopy shows multiple vascular abnormalities in the jejunum . Which of the following is the most like diagnosis?
. Dieulafoy’s lesions
Anemia from chronic renal failure
Vascular ectasia
Crohn’s disease
Small bowel diverticulosis
Question 47. A 68-year-old man presents with intermittent episodes of hematochezia for several months. His stools are normal, but he passes blood clots a few times per week. His past medical history is significant for prostate cancer, for which he received radiation therapy 4 years ago. He denied any weight loss or diarrhea. Physical examination is unremarkable. An endoscopic view of the rectum showed: rectum appears with friability and telangiectasia pale. These findings are limited to the distal rectum. Which of the following is the most likely diagnosis?
Hereditary hemorrhagic telangiectasia
Ulcerative proctitis
Ischemic colitis
Crohn’s colitis
Radiation proctopathy
48. A 28-year-old woman with a history of an appendectomy presents with a non-tender palpable mass in the right lower quadrant abdominal incision. The following statement(s) is/are true concerning the diagnosis and management of this patient.
The best diagnostic test involves imaging of the abdominal wall by either CT or MRI
Resection of the mass with a 2 cm margin is usually adequate
Low dose radiation is a suitable alternative to surgery for primary treatment
Re-resection for recurrence will likely have a higher rate of recurrence than for primary resection
Therapeutic endoscopic should be an option for the treatment of the mass.
49. The following statement about peritonitis are all true except:
Peritonitis is defined as inflammation of the peritoneum.
Most surgical peritonitis is secondary to bacterial contamination
Primary peritonitis no documented source of contamination and is more common in adults than in children and in men than in has women.
Tuberculous peritonitis can present with or without ascites.
Cirrhotic ascites can complicate to peritonitis
50. Acute appendicitis is most commonly associated with which of the following signs?
Temperature above 104؛ F.
Frequent loose stools.
Anorexia, abdominal pain, and right lower quadrant tenderness.
White blood cell count greater than 20,000 per cu. mm.
Anuria, hypothermy, constipation
51. Which of the following most often initiates the development of acute appendicitis?
A viral infection.
Acute gastroenteritis.
Obstruction of the appendiceal lumen.
. A primary clostridial infection.
Therapeutic colonoscopy
52. The best type of x-ray to locate free abdominal air is:
A posteroanterior view of the chest.
. A flat and upright view of the abdomen.
. Computed tomograph (CT) of the abdomen.
A lateral decubitus x-ray, right side up.
Plain X-Ray on the bed of the patient
53. The most helpful diagnostic radiographic procedure in small bowel obstruction is:
. CT of the abdomen.
Contrast study of the intestine.
Supine and erect x-rays of the abdomen
. Ultrasonography of the abdomen.
MRI of abdomen.
54. The most commonly used imaging method for diagnosis of acute cholecystitis is:
CT of the abdomen
Ultrasonography of the gallbladder
Oral cholecystogram
Radionuclide (HIDA) scan of the gallbladder
Endoscopic ultrasound
55. Meckel's diverticulitis most often occurs in the:
Proximal jejunum.
Distal jejunum.
Proximal ileum.
Distal ileum.
Proximal colon
56. Of adult patients presenting to the emergency room for evaluation of acute abdominal pain, which one of the following answers includes the most common diagnoses?
Urologic problems, cholelithiasis, pelvic inflammatory disease
Mittelschmerz, appendicitis, ureterolithiasis
Nonspecific abdominal pain, appendicitis, intestinal obstruction
Appendicitis, pelvic inflammatory disease, perforated ulcer
Ectopic pregnancy complication
57. Visceral pain is typically:
Well localized
Sharp
Mediated via spinal nerves
Perceived to be in the midline
Burning
58. A 26-year old woman in her first trimester of pregnancy presents with a 2-day history of right lower quadrant pain and fever. Physical examination reveals a tender, palpable, right lower quadrant mass. There is no evidence of peritonitis or systemic sepsis. Laboratory evaluation is remarkable for mild leukocytosis, and abdominal ultrasound demonstrates an inflammatory mass but no evidence of abscess. As the surgeon on call, your recommendation would be:
Intravenous hydration, antibiotic prophylasis, and urgent appendectomy
Intravenous hydration, antibiotics, bowel rest, and interval appendectomy in 4 to 6 weeks
Intravenous hydration, antibiotics, and appendectomy if no improvement in 12 to 24 hours
Intravenous hydration, antibiotics, and interval appendectomy when fever has subsided, leukocyte count has returned to normal, and the patient is pain free
Emergent obstetrical consultation for evaluation and treatment of possible ectopic pregnancy
59. True statements regarding appendiceal neoplasms include which of the following?
Carcinoid tumors of the appendix less than 1.5 cm are adequately treated by simple appendectomy
Appendiceal carcinoma is associated with secondary tumors of the GI tract in up to 60% of patients
Survival following right colectomy for a Dukes’ stage C appendiceal carcinoma is markedly better than that for a similarly staged colon cancer at 5 years
Mucinous cystadenocarcinoma of the appendix is adequately treated by simple appendectomy, even in patients with rupture and mucinous ascites
Up to 50% of patients with appendiceal carcinoma have metastatic disease, with the liver as the most common site of spread
60.Gastro-oesophageal reflux can reliably be diagnosed by
Symptoms
Biopsy histology of the gastro-oesophageal junction
Manometry
24 hour pH monitoring
. Bernstein test
61)Which of the following statements about the anatomic course of the esophagus is correct?
The cervical esophagus passes behind and to the right of the trachea.
The thoracic esophagus enters the posterior mediastinum anterior to the aortic arch.
The thoracic esophagus passes behind the right mainstem bronchus and the pericardium
The esophagus enters the diaphragmatic hiatus at the level of T8.
The esophagus deviates anteriorly and to the left as it enters the abdomen.
62). Which of the following statements about esophageal anatomy is correct?
The esophagus has a poor blood supply, which is segmental in distribution and accounts for the high incidence of anastomotic leakage
The esophageal serosa consists of a thin layer of fibroareolar tissue.
The esophagus has two distinct muscle layers, an outer, longitudinal one and an inner, circular one, which are striated in the upper third and smooth in the distal two thirds.
. Injury to the recurrent laryngeal nerve results in vocal cord dysfunction but does not affect swallowing.
The lymphatic drainage of the esophagus is relatively sparse, localized primarily to adjacent paraesophageal lymph nodes.
63). Which of the following statements about the lower esophageal sphincter (LES) mechanism, or high-pressure zone (HPZ), is true?
The LES is a circular smooth muscle ring that is 3 to 5 cm. long.
In assessing esophageal manometric data, mean HPZ pressure less than 6 mm. Hg or overall length less than 2 cm. Is more likely to be associated with incompetence of the LES and gastroesophageal reflux
Esophageal manometry and the acid perfusion (Bernstein) test reliably identify the patient with an incompetent LES mechanism
Distal HPZ relaxation occurs within 5 to 8 seconds of initiating a swallow.
Twenty-four–hour distal esophageal pH monitoring is achieved with an intraesophageal pH electrode positioned at the esophagogastric junction.
64. Which of the following statements about achalasia is/are correct?
In most cases in North America the cause is a parasitic infestation by Trypanosoma cruzi.
Chest pain and regurgitation are the usual symptoms
Distal-third esophageal adenocarcinomas may occur in as many as 20% of patients within 10 years of diagnosis.
Manometry demonstrates failure of LES relaxation on swallowing and absent or weak simultaneous contractions in the esophageal body after swallowing
Endoscopic botulinum toxin injection of the LES, pneumatic dilatation, and esophagomyotomy provide highly effective curative therapy for achalasia.
65. Which of the following statements about epiphrenic diverticula of the esophagus is/are correct?
They are traction diverticula that arise close to the tracheobronchial tree.
They characteristically arise proximal to an esophageal reflux stricture.
The degree of dysphagia correlates with the size of the pouch.
They are best approached surgically through a right thoracotomy.
The operation of choice is a stapled diverticulectomy, long esophagomyotomy, and partial fundoplication
66. Which of the following statements about Schatzki's ring is correct?
The ring represents a panmural fibrotic stricture resulting from gastroesophageal reflux.
Dysphagia occurs when the ring diameter is 13 mm. Or less
The ring occurs within 1 to 2 cm. Of the squamocolumnar epithelial junction
Schatzki's ring indicates reflux esophagitis
Schatzki's ring signifies the need for an antireflux operation.
67. Which of the following statements about pathology encountered at esophagoscopy is/are correct?
Reflux esophagitis should be graded as mild, moderate, or severe, to promote consistency among different observers.
An esophageal reflux stricture with a 2-mm. Lumen is not dilatable and is best treated with resection.
A newly diagnosed radiographic distal esophageal stricture warrants dilation and antireflux medical therapy.
In patients with Barrett's mucosa, the squamocolumnar epithelial junction occurs 3 cm. Or more proximal to the anatomic esophagogastric junction
After fasting at least 12 hours, a patient with megaesophagus of achalasia can safely undergo flexible fiberoptic esophagoscopy
68. Which of the following statements about the diagnosis and treatment of esophageal leiomyomas is/are correct?
The majority are diagnosed after they cause dysphagia and chest pain.
. Biopsy is indicated at the time of esophagoscopy, to rule out carcinoma.
Full-thickness elliptical excision of the esophageal wall is the preferred surgical approach.
Endoscopic ultrasonography is a reliable means of following leiomyomas conservatively
. Recurrence of resected leiomyomas is minimized by wide local excision.
69. Which of the following statements regarding the pathology of esophageal carcinoma is/are correct?
Worldwide, adenocarcinoma is the most common esophageal malignancy.
Squamous cell carcinoma is most common in the distal esophagus, whereas adenocarcinoma predominates in the middle third.
Patients with Barrett's metaplasia are 40 times more likely than the general population to develop adenocarcinoma
Metastases from esophageal carcinoma are characteristically localized to regional mediastinal lymph nodes adjacent to the tumor.
Achalasia, radiation esophagitis, caustic esophageal stricture, Barrett's mucosa, and Plummer-Vinson syndrome are all premalignant esophageal lesions that predispose to the development of squamous cell carcinoma
70. Which of the following statements about the surgical treatment of esophageal carcinoma is/are correct?
. The finding of severe dysphagia in association with Barrett's mucosa is an indication for an antireflux operation to prevent subsequent development of carcinoma.
. Long-term survival is improved by radical en bloc resection of the esophagus with its contained tumor, adjacent mediastinal tissues, and regional lymph nodes.
The morbidity and mortality rates for cervical esophagogastric anastomotic leak are substantially less than those associated with intrathoracic esophagogastric anastomotic leak
The leading complications of transthoracic esophagectomy and intrathoracic esophagogastric anastomosis are bleeding and wound infection.
Transhiatal esophagectomy without thoracotomy achieves better long-term survival than transthoracic esophagectomy.
71. The best management for a 48-hour-old distal esophageal perforation is:
Antibiotics and drainage
Division of the esophagus and exclusion of the perforation.
Primary repair with buttressing
Resection with cervical esophagostomy, gastrostomy, and jejunostomy.
T-tube fistula and drainage.
72. A 50-year-old patient develops sudden left lower chest pain and epigastric pain after vomiting. The patient shows diaphoresis, breath sounds are decreased on the left, and there is abdominal guarding. The most appropriate diagnostic test is:
Aortography.
Esophagoscopy.
Electrocardiogram.
Film of the chest
White blood count.
73.The following statements about the influence of diet and lifestyle on lower esophageal sphincter (LES) function are true except one. Identify the incorrect statement.
A high-protein diet increases LES pressure
A fat meal results in sustained decrease in LES pressure.
Chocolate ingestion causes a decrease in LES pressure
. Peppermint produces a transient decrease in LES values.
Cigarette smoking produces no significant changes in LES pressures
74. When a stricture is present in association with gastroesophageal reflux, each of the following is an acceptable repair for reflux control except one. Identify the poorest repair.
Intrathoracic total fundoplication.
. Lengthening gastroplasty with total fundoplication
Total fundoplication
Lengthening gastroplasty with partial fundoplication.
Partial fundoplication
75. When assessing gastroesophageal reflux disease by manometry each of the following statements is correct except one. Identify the incorrect one.
Absent or extremely low LES pressures have predictive value in identifying more severe reflux.
Peristaltic dysfunction increases with increasing severity of esophagitis.
With established reflux disease the UES is hypertensive
. Esophageal functional changes are worst in patients with a circumferential columnar-lined esophagus.
Absence of peristalsis may be associated with more severe forms of reflux disease.
76. The presence of a nonmalignant mid- or upper esophageal stricture always indicates the presence of:
Alkaline reflux esophagitis.
Barrett's esophagus
Idiopathic reflux disease
Mediastinal fibrosis.
Scleroderma.
77. Which of the following is most reliable for confirming the occurrence of a significant esophageal caustic injury?
History of the event.
Physical examination of the patient
Barium esophagraphy.
Endoscopy
Manometry
78. First-line therapy for routine peptic duodenal ulcer disease includes:
Vagotomy and antrectomy
Upper endoscopy and biopsy to rule out tumor.
Evaluation for Helicobacter pylori
Serum gastrin determination.
Cream or milk-based “Sippy” diet.
79. Appropriate management of severe vomiting associated with gastric outlet obstruction from peptic ulcer disease includes all of the following except:
Nasogastric suction.
Intravenous hydration.
. Nutritional assessment; upper endoscopy to rule out malignancy
Intravenous H 2 antagonist.
Oral antacid therapy
80. Secretion of gastric juice is stimulated by
Enterogastrin
Gastrin
Cholecystokini
Non of enterogastrin, gastrin, cholecystokine
Prostaglandin
81. Bile acts as activator of which enzyme
Lipase
Pepsinogen
Pancreatic amylase
Trypsinogen
Glucagon
82. HCI of the gastric juice
Activates both pepsin and ptyalin
Inactivates both pepsin and ptyalin
Activates pepsin and inactivates ptyalin
Activates ptyalin and inactivates pepsin
Activatea gastrin
83. Cholecystokinin stimulates
Pancreas
Gall bladder
Gastric gland
None of pancreas, gall bladder, gastric gland
Brunner’ s gland
84. Brunner’s glands are present in
Stomach
Ileum
Duodenum
Oesophagus
Colon
85. Crypts of Lieberkuhn are present in
Intestine
Stomach
Oesophagus
Intestine, stomach, oesophagus
Colon
86. Oxyntic cells secrete
Trypsin
HCI
NaoH
Pepsin
Mucous
87. The hepatic cells which act as phagocytes are
Kuffer cells
Acinar cells
Hansen’s cells
Ito cell
Fibroblaste
100) Which of the following is the most important goal of treating chronic viral hepatitis C infection
Normalie ALT and AST.
Improve symptoms.
Reverse cirrhosis.
Eliminate the HCV RNA from serum
Seroconversion Ac HCV
101) What specific treatment do you recommend for chronic hepatitis C infection for TAS
Interferon- ribavirin
Lamivudine
Sofosbuvir and Ribavirin
Sofosbuvir and Ledispavir.
Peg-interferon and Ribavirin
103) A nurse sustains a needle stick from a patient who is known to be HBsAg-positive. She has been vaccinated previously with hepatitis B vaccine and is a known nonresponder. What post-exposure prophylaxis should the nurse receive?
One dose of HBIG and one dose of hepatitis B vaccine
Give the nurse Tenofovir for 30 days
One dose of hepatitis B vaccine
Test the nurse for anti-HBs level and treat accordingly
Give the nurse double dose of vaccine
105) Hepatitis D is commonly associated with what other type of viral hepatitis
Hepatitis E
Hepatitis C
Hepatitis B
Hepatitis G
Hepatitis B and C
109) The disease exists in short-term (acute) and long-term (chronic) forms. How long does acute hepatitis last?
Less than 6 months
. Less than 3 months
About 6 weeks
1 month
1 year
111). Which form of hepatitis can be passed on through contaminated food or water?
. B
C
A and E
B and C
D
113). Vaccines have been developed to protect against which hepatitis viruses?
Hepatitis A virus
Hepatitis B virus
Hepatitis D virus
Hepatitis A and hepatitis B virus
Hepatitis C virus
114. A 28-year-old woman with a history of an appendectomy presents with a non-tender palpable mass in the right lower quadrant abdominal incision. The following statement(s) is/are true concerning the diagnosis and management of this patient.
The best diagnostic test involves imaging of the abdominal wall by either CT or MR
Resection of the mass with a 2 cm margin is usually adequate
Low dose radiation is a suitable alternative to surgery for primary treatment
Re-resection for recurrence will likely have a higher rate of recurrence than for primary resection
Therapeutic endoscopic should be an option for the treatment of the mass.
118. The following statement about peritonitis are all true except:
Peritonitis is defined as inflammation of the peritoneum
Most surgical peritonitis is secondary to bacterial contamination
Primary peritonitis has no documented source of contamination and is more common in adults than in children and in men than in women
Tuberculous peritonitis can present with or without ascites.
Cirrhotic ascites can complicate to peritonitis
119. Acute appendicitis is most commonly associated with which of the following signs?
Temperature above 104؛ F.
Frequent loose stools.
Anorexia, abdominal pain, and right lower quadrant tenderness
White blood cell count greater than 20,000 per cu. mm.
Anuria, hypothermy, constipation
120. Which of the following most often initiates the development of acute appendicitis?
. A viral infection.
Acute gastroenteritis.
Obstruction of the appendiceal lumen
A primary clostridial infection
Therapeutic colonoscopy
123. The best type of x-ray to locate free abdominal air is:
A posteroanterior view of the chest
A flat and upright view of the abdomen
Computed tomograph (CT) of the abdomen
A lateral decubitus x-ray, right side up.
Plain X-Ray on the bed of the patient
124. The most helpful diagnostic radiographic procedure in small bowel obstruction is:
CT of the abdomen.
Contrast study of the intestine
Supine and erect x-rays of the abdomen
Ultrasonography of the abdomen
MRI of abdomen.
125. The most commonly used imaging method for diagnosis of acute cholecystitis is:
CT of the abdomen.
Ultrasonography of the gallbladder
Oral cholecystogram.
Radionuclide (HIDA) scan of the gallbladder.
Endoscopic ultrasound
126. Meckel's diverticulitis most often occurs in the:
Proximal jejunum
Distal jejunum.
Proximal ileum.
Distal ileum
Proximal colon
127. Of adult patients presenting to the emergency room for evaluation of acute abdominal pain, which one of the following answers includes the most common diagnoses?
Urologic problems, cholelithiasis, pelvic inflammatory disease
Mittelschmerz, appendicitis, ureterolithiasis
Nonspecific abdominal pain, appendicitis, intestinal obstruction
. Appendicitis, pelvic inflammatory disease, perforated ulcer
Ectopic pregnancy complication
131. Visceral pain is typically
Well localized
Sharp
Mediated via spinal nerves
. Perceived to be in the midline
Burning
133. A 26-year old woman in her first trimester of pregnancy presents with a 2-day history of right lower quadrant pain and fever. Physical examination reveals a tender, palpable, right lower quadrant mass. There is no evidence of peritonitis or systemic sepsis. Laboratory evaluation is remarkable for mild leukocytosis, and abdominal ultrasound demonstrates an inflammatory mass but no evidence of abscess. As the surgeon on call, your recommendation would be:
Intravenous hydration, antibiotic prophylasis, and urgent appendectomy
Intravenous hydration, antibiotics, bowel rest, and interval appendectomy in 4 to 6 weeks
Intravenous hydration, antibiotics, and appendectomy if no improvement in 12 to 24 hours
Intravenous hydration, antibiotics, and interval appendectomy when fever has subsided, leukocyte count has returned to normal, and the patient is pain free
Emergent obstetrical consultation for evaluation and treatment of possible ectopic pregnancy
134. True statements regarding appendiceal neoplasms include which of the following?
Carcinoid tumors of the appendix less than 1.5 cm are adequately treated by simple appendectomy
. Appendiceal carcinoma is associated with secondary tumors of the GI tract in up to 60% of patients
Survival following right colectomy for a Dukes’ stage C appendiceal carcinoma is markedly better than that for a similarly staged colon cancer at 5 years
Mucinous cystadenocarcinoma of the appendix is adequately treated by simple appendectomy, even in patients with rupture and mucinous ascites
Up to 50% of patients with appendiceal carcinoma have metastatic disease, with the liver as the most common site of spread
135. Un homme de 62 ans vous voyez en consultation pour une trouble du transite récente. Il se plaint d’avoir une constipation depuis environs 2 mois. Le symptôme s’est aggravé depuis environs 2 semaines. A l’interrogatoire vous notez des épisodes de rectorrhagie minime depuis environs 2 mois et une notion de perte de poids de 5 kg en 2 mois. Cliniquement, le ventre est souple, pas de masse palpable. Quel est le diagnostic le plus probable?
A. Constipation chronique
B. Trouble fonctionnelle intestinale
C. Cancer colorectal
D. Hémorroïde
E. Hypothyroïdie
136. Un homme de 67 ans vous voyez en consultation pour une rectorrhagie. Il se plaint d’avoir des épisodes de rectorrhagie depuis environs 6 mois. Il n’y pas de douleur ou de trouble du transit. A l’interrogatoire vous notez des épisodes de rectorrhagie minime parfois émission de caillots de sang par l’anus. Cliniquement, le ventre est souple, pas de masse palpable. Les conjonctives sont pâles. Le pouls est de 96/mn. Quel l’examen demandez vous pour confirmer le diagnostique?
A. Examen proctologique
B. Recto-sigmoïdoscopie
C. Echographie abdominale
D. Scanner abdomino-pelvienne
E. Coloscopie totale
137. Une coloscopie chez un patient de 55 ans retrouve une tumeur moyenne rectum biopsiée, l’anatomo-pathologie retrouve un adénocarcinome lieberkühnien. Quel est votre bilan d’extension ?
A. TDM thoraco-abdomino-pelvienne
B. PET TDM
C. Radiographie pulmonaire
D. IRM abdomino-pelvienne
E. Echographie abdominale
138. Une femme de 58 ans admise au service d’hépatogastroentérologie pour suspicion cancer du colon. Elle se plaint d’avoir une constipation depuis environ 1 mois et le symptôme semble aggraver depuis environs 2 semaines. Elle a l’ATCD de lithiase de la vésicule biliaire et alcoolisme chronique. Après avoir bu 2 litres de Fortran pour la préparation colique, elle se plaint de douleur abdominale assez importante avec le ventre très ballonné. Quel diagnostic évoquez-vous ?
A. Occlusion du intestinale
B. Perforation colique
C. Ischémie mésentérique
D. Pancréatite aiguë
E. Cholécystite aiguë
139. Au cours d'une occlusion par cancer sténosant du sigmoïde :
A. Les vomissements sont précoces
B. L’ 'arrêt des matières et des gaz est tardif
C. L'angle colique gauche est distendu
D. Le toucher rectal fait le diagnostic
E. L’abdomen est mat à la percussion
140. Parmi les données de l'examen histopathologique d'une pièce opératoire de cancer du colon ou du rectum qui ont une influence sur le pronostic, on peut citer :
A. Le caractère circonférentiel de la lésion
B. Le niveau d'invasion selon Astler et Coller
C. Le caractère infiltrant de la lésion
D. Le cancer développé sur polype
E. L'atteinte ganglionnaire
141. Quelle est l'attitude thérapeutique à proposer chez un homme de 50 ans, en bon état général chez lequel le bilan d'extension d'un cancer du rectum à 4 cm de la marge anale découvre une métastase hépatique unique superficielle du segment VI de 2 cm de diamètre ?
A. Dérivation colique et chimiothérapie
B. Irradiation pelvienne et chimiothérapie
C. Radiothérapie de contact et chimiothérapie
D. Amputation abdomino-périnéale et métastasectomie
E. Amputation abdomino-périnéale et chimiothérapie intra-hépatique
142. Un cancer du rectum T3 N1 M0 en bilan pré-opératoire nécessite un traitement adjuvant par une seule méthode avant l'intervention. Laquelle?
A. Curiethérapie
B. Radiothérapie et chimiothérapie intensive
C. Radiothérapie avec 5 FU potentialisant l'effet de la radiothérapie
D. Chimiothérapie associant 5 FU, Cisplatyl, acide folinique
E. Aucune de ces propositions n'est exacte
143. La surveillance du cancer du côlon après résection chirurgicale à visée curative comporte pendant les 3 premières années : (quelle est la proposition exacte?)
A. Un dosage du CA 19-9 tous les 3 mois
B. Une tomodensitométrie abdomino-pelvienne tous les 3 à 6 mois
C. Une immuno-scintigraphie par anticorps monoclonaux pour repérage de l'ACE tumoral
D. Une coloscopie tous les 3 à 6 mois
E. Une échographie tous les 3 à 6 mois
144. Un homme de 45 ans vient de subir une résection antérieure pour un adénocarcinome du rectum situé à 8 cm de la marge anale. L'examen anatomo-pathologique conclut à un stade pT1 pNO MO (envahissement de la sous-muqueuse). Quelle attitude complémentaire faut-il programmer?
A. Association chimiothérapie-radiothérapie
B. Immunothérapie active non spécifique
C. Irradiation pelvienne
D. Surveillance clinique et endoscopique
E. Aucune de ces attitudes
145. Vous voyez en consultation une femme de 60 ans une douleur HCD minime intermittente depuis environs 6 mois. La tempţérature est de 38oC mais il n’y a pas d’ictère. L’examen physique montre une douleur HCD minime à la palpation. Elle n’a pas ATCD particulier. Echographie abdominal est demandée et montre une épaississement et irrégularité de la paroi vésiculaire. Quel est le diagnostic le plus probable ?
Cholécystite aiguë lithiasique
Cholécystite aiguë alithiasique
Cholécystite chronique
Cancer de la vésicule biliaire
Abcès de la vésicule biliaire
146. Une femme de 45 ans consulte pour un ictère fébrile. La Température est à 39oC. La TA est à 100/60 mmHg, le pouls est à 110/mm. L’examen biologique montre : GB 20 Giga/L, CRP 200 mg/l, ASAT 60 UI/L, ALAT 120 UI/L, PAL 300 UI/L, GGT 122 UI/L, Bili T 100mg/L, Bili D 45mg/L. Quel examen de première intension demandez-vous pour confirmer le diagnostic ?
ASP
Échographie abdominale
Scanner abdominal
IRM
CPRE
147. Une femme de 38 ans, obèse, admise au Urgence pour une douleur HCD, fièvre et ictère. Ses symptômes commencent depuis environs 3 jours. À l’interrogatoire, elle vous révèle que la douleur survienne brutalement et s’aggrave à l’inspiration profonde. L’examen physique montre un signe de Murphy positive. Quel est le diagnostic le plus probable ?
Cholécystite aiguë lithiasique
Angiocholite lithiasique
Pancréatite aiguë
Abcès du foie
Colique hépatique
148. Une femme de 45 ans sans antécédent particulier vient vous voir pour le bilan de santé. L’échographie abdominale montre un calcul de 10 mm dans la vésicule biliaire. Elle n’a ni fièvre ni douleur. L’examen physique est complètement normal. Quel traitement proposez-vous ?
Cholecystectomie
CPRE avec sphincterotomie
Abstention thérapeutique
Antibiothérapie
Traitement médical
149. Une femme de 45 ans sans antécédent particulier vient vous voir pour le bilan de santé. Elle est complètement asymptomatique. L’examen physique est complètement normal. L’échographie abdominale montre une vésicule biliaire scléro-atrophique. Quel traitement proposez-vous ?
Cholecystectomie
Surveillance échographique
Abstention thérapeutique
Antibiothérapy
CPRE avec sphincterotomie
150. Un home de 50 ans, obèse, vient vous voir en consultation spécialisé pour une vésicule de porcelaine ayant découverte fortuitement sur un bilan de santé. Il est complètement asymptomatique. Son médecin lui demande d’opérer, mais il a peur de l’opération. Il veut savoir votre avis. Quel est le risque s’il n’opère pas ?
Cholécystite aiguë lithiasique
Angiocholite lithiasique
Pancréatite aiguë
Abcès du foie
Cancer de la vésicule biliaire
151. Un homme de 45 ans, se présence aux urgences pour douleurs abdominales survenues brutalement il y a quelques heures. Il s’agit de douleurs épigastriques intenses (EVA à 8) avec irradiation postérieure associées à 2 épisodes de vomissements alimentaire. Le diagnostique de pancréatite aiguë est confirmé. Le scanner de 48 heures est réalisé. Quelle est la proposition juste ?
A. A = Foie, B = Pancréas, C = Intestin grêle
B. A= Foie, B = vésicule biliaire, C = Pancréas
C. A = Foie, B = Intestin grêle, C = Pancréas
D. A = Rate, B = Intestin grêle, C = Pancréas
E. A = Rate, B = Pancréas, C = Intestin grêle
152. Un homme de 40 ans, se présence aux urgences pour douleurs abdominales survenues brutalement il y a quelques heures. Il s’agit de douleurs épigastriques intenses (EVA à 7) avec irradiation postérieure associées à 2 épisodes de vomissements alimentaires. Elles sont soulagées par la position en chien de fusil. Il est alcoolisme chronique. Pas d’autres antécédents notables. Quel est le bilan biologique le plus approprié pour confirmer le diagnostique de pancréatite aiguë ?
A. Lipasémie > 3N
B. Amylasémie > 3N
C. Lipasémie > 2N
D. Amylasémie > 2N
E. Triglycéridémie > 15g/dl
153. Une femme de 40 ans, obèse, se plaint de douleurs sus ombilicale à prédominant HCD survenue brutalement depuis environs 4 heures. La douleur est intense (EVA à 8) avec irradiation postérieure. Dans ses ATCD on note : HAT (-), daibète (-), Alcool (-), Tabac (-), cholécystectomie pour une cholécystite aiguë il y a 2 mois. ECG réalisé en urgence est normale. Quel est le diagnostique le plus probable ?
A. Infarctus du myocarde
B. Angiocholite lithiasique
C. Ulcère gastrique
D. Pancréatite aiguë lithiasique
E. Infarctus mésentérique
154. Un homme de 38 ans, alcoolisme chronique active, se présence aux urgences pour douleurs abdominales survenues brutalement il y a quelques heures. Il s’agit de douleurs épigastriques intenses (EVA à 8) avec irradiation postérieure associées à 2 épisodes de vomissements alimentaires. Elles sont soulagées par la position en chien de fusil. Il est alcoolisme chronique. Pas d’autres antécédents notables. Le diagnostique de pancréatite aiguë est confirmé. Quel est le bilan biologique le plus simple pour évaluer la gravité de ce patient ?
A. CRP > 150
B. CRP > 50
C. Lipasémie > 7 N
D. Lipasémie > 10 N
E. Hématocrite < 40 %
{"name":"HGE", "url":"https://www.quiz-maker.com/QPREVIEW","txt":". For patients with diagnosis as dyspepsia, they may have many symptoms. Which of the following symptoms is the most likely encountered?, . For the patient you consult for dyspepsia, you have to do anamnesis and clinical examination to find the causes. Which of the following etiology that is the most likely play a role?, Some drugs can cause dyspepsia. So during your anamnesis for patient with dyspepsia, you have to think of some drug name. What medication is the most likely responsible?","img":"https://cdn.poll-maker.com/10-464155/untitled.png?sz=1200"}
More Quizzes
Whos the best couple
100
Answer
7428
Adult or Broken?
840
Do you know ennard the best
1160
Making Fashion: Apparel Design in Context
15819890
Free Anatomy and Physiology Knowledge Test
201021661
Ultimate Asterix Character: Name Your Gaulish Heroes
201040482
Ace the Biology 101 Lab Practical - Test Your Skills
201030535
Discover Your Perfect Boyfriend From Stranger Things!
201023909
Quiz La France: Défiez Vos Connaissances Françaises !
201083044
Ultimate SpongeBob: Can You Name SpongeBob's Pet Worm?
201030898
Free Multiplication Fluency Assessment
201029179